How do you write a soap report?
How do you write a soap report?
Tips for Effective SOAP Notes
- Find the appropriate time to write SOAP notes.
- Maintain a professional voice.
- Avoid overly wordy phrasing.
- Avoid biased overly positive or negative phrasing.
- Be specific and concise.
- Avoid overly subjective statement without evidence.
- Avoid pronoun confusion.
- Be accurate but nonjudgmental.
What does soap mean in charting?
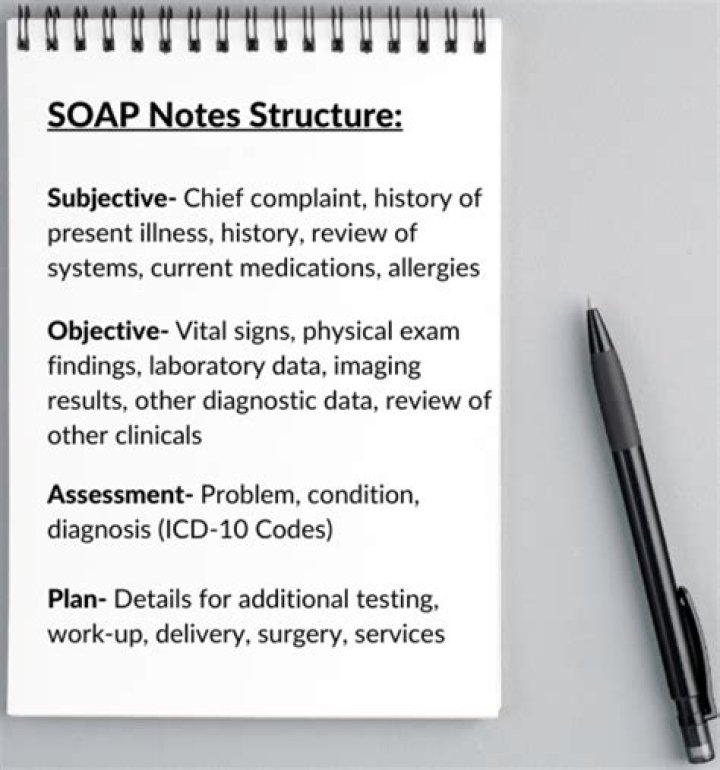
Subjective, Objective, Assessment and Plan
Introduction. The Subjective, Objective, Assessment and Plan (SOAP) note is an acronym representing a widely used method of documentation for healthcare providers.
What is the assessment in SOAP notes?
Assessment: The next section of a SOAP note is assessment. An assessment is the diagnosis or condition the patient has. In some instances, there may be one clear diagnosis.
What is soap format of assessment?
The SOAP note (an acronym for subjective, objective, assessment, and plan) is a method of documentation employed by healthcare providers to write out notes in a patient’s chart, along with other common formats, such as the admission note.
How is a SOAP note used?
Today, the SOAP note – an acronym for Subjective, Objective, Assessment, and Plan – is the most common method of documentation used by providers to input notes into patients’ medical records. They allow providers to record and share information in a universal, systematic and easy-to-read format.
How do I make a SOAP document?
S.O.A.P.S. Document Analysis
- Speaker. Who is the speaker who produced this piece? What is the their background and why are they making the points they are making?
- Occasion. What is the Occasion?
- Audience. Who is the Audience?
- Purpose. What is the purpose?
- Subject. What is the subject of the document?
How do you write the assessment part of a SOAP note?
How to Write a SOAP Note Following the SOAP Note Format?
- Subjective – What the Patient Tells you. This section refers to information verbally expressed by the patient.
- Objective – What You See.
- Assessment – What You Think is Going on.
- Plan – What You Will Do About It.
What is objective in SOAP notes?
The Objective (O) part of the note is the section where the results of tests and measures performed and the therapist’s objective observations of the patient are recorded. Objective data are the measurable or observable pieces of information used to formulate the Plan of Care.